What is Positional Plagiocephaly or 'Flat Head Syndrome'?
It typically appears before an infant is 20 weeks old and can dramatically affect the shape of a baby’s head. Also known as deformational plagiocephaly or flat head syndrome, it is caused by the baby being in the same position for an extended amount of time (a crib, car seat carrier, swing).
Sometimes, this condition can be noticed while carrying the baby, the head may feel like it has an irregular shape/ asymmetry. A bald spot may also appear in the area where the infant prefers to rest his or her head. Also, the hair in the area might not lie flat, with hair strands extending outward instead of lying smoothly against the head. When asymmetry is mild to moderate, changes in sleep positioning and activities may help to improve the skull shape without the need for further intervention. Infants with more severe cranial asymmetry may have a chance for improvement and benefit from cranial remodeling treatment with helmet therapy.
Since 1996, the American Academy of Pediatrics (AAP) recommends that babies sleep on their back to reduce the risk of Sudden Infant Death Syndrome (SIDS). Parents are encouraged to always check with their pediatrician first for guidance.
It is recommended that all infants with cranial asymmetry be properly evaluated by a pediatric cranial specialist to rule out craniosynostosis. Unlike positional plagiocephaly, craniosynostosis requires surgery and can be diagnosed by X-ray.
Treatments and Procedures
- Plastic surgery evaluation
- Referrals to diagnostic imaging, certified orthotics and physical therapy as needed.
Treatments and Procedures
The members of the
Craniofacial team work together to develop and deliver a coordinated plan of care to meet each child’s individual needs. The team’s plastic surgeons are physicians who have extensive experience with children who have craniofacial differences.
Conditions We Treat
How does positional plagiocephaly differ from craniosynostosis?
Most children with cranial asymmetry simply have positional plagiocephaly. However, some infants are born with craniosynostosis, which unlike positional plagiocephaly, requires surgical intervention. Differentiating positional plagiocephaly from craniosynostosis is done primarily by physical examination, followed by radiographic confirmation. Look for these signs to recognize the difference:
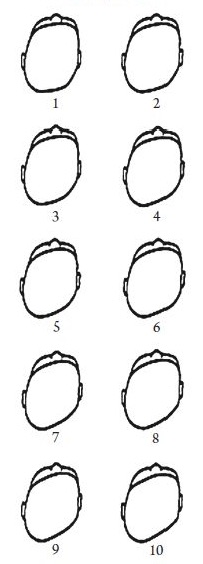
Severity Scale for Positional Plagiocephaly
Signs of Craniosynostosis
Coronal Synostosis (Left Sided)
– Ear anterior on side of flattened forehead.
– Nose deviated to contralateral side.
– Eye on affected side appears larger, known as "Harlequin eye".
– Stabismus present in 30% of patients.
Lambdoid Synostosis (Right Sided)
– Cranium has a trapezoidal shape.
– Ear is more posterior on side of flattened occiput.
– A mastoid bulge is present on the affected side.
– Contralateral frontal bossing.
Metopic Synostosis
– Triangular shaped brow.
– Eyes appear closely set.
– Mild cases may only have a forehead ridge.
Sagittal Synostosis
– Long and narrow head.
– May have frontal bossing.
– May have occipital prominence.
– Head circumference is usually greater than 90%