Conventional MR images are two-dimensional representation of intensities occurring at a given level or slice.
These images may be presented in axial, coronal and sagittal planes.
The most frequent plane used in fMR is the axial plane which shows the localization of structures or activation in a X (right to left) and a Y (anterior to posterior) axes. Since these images are usually obtained in oblique planes it is difficult to know the precise level in the remaining Z (cranio-caudal) axis.
3D MRI scans allow us to present images with a volumetric appearance. These 3D MRI images have proven to be useful to guide surgical resections.
Types of 3D MRI scans
Orthogonal Views
Orthogonal views refer to a set of mutually perpendicular images. This localizes a given region of activation to the three axes that define the volumetric shape of the brain.
Case 1
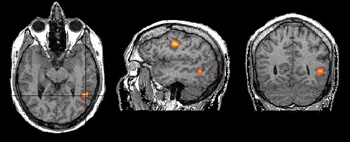
Adult volunteer generating verbs. On the axial view the exact location of activation in the temporal lobe is difficult to determine. The black lines in the axial view correspond to the location of the coronal and sagittal views. These three views allow us to determine the location of activation in the middle temporal gyrus.
Case 2
Right handed adult male patient with intractable seizures coming from the left temporal pole, performing a language task consisting of listening to a story. No structural lesion was found in this region. A left temporal resection is planned. The orthogonal views permit evaluating of the extent of the language areas and the distance between its anterior border and the temporal pole (orange line). The neurosurgeon may use these findings as a guide to tailor the temporal resection.
Surface Rendering
Surface rendering is a computer post processing method that removes the skin and the skull to allow us to see the brain surface. The anatomy of gyri and sulci are displayed in the same way the neurosurgeon sees the brain. Functional maps can be superimposed on these images. Some activation may take place deep in the sulci which may be presented on these images bleeding through the cortical surface.
Case 1
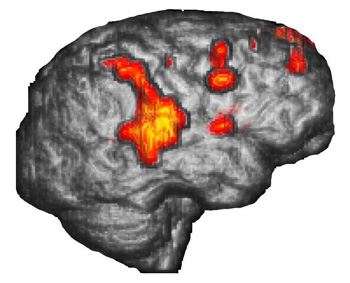
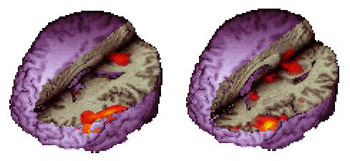
Right handed 15 year-old-boy with intractable epilepsy performing a verbal "repetition task." The surface rendition beautifully depicts the activation occurring in the posterior third of the right superior temporal gyrus and extending toward supramarginal gyrus and Brodmann's area 7. The areas of activation are better displayed than with conventional 2D MR images.
Case 2
Right handed 11 year-old-girl with intractable epilepsy who had a left frontal resection two years ago for control of seizures. Persistence of the seizures prompted this fMR exam for re-evaluation. The images demonstrated activation obtained from a "Verb Generation Task." The study depicted Broca's area and part of Wernicke's (Brodmann's area 37), which is believed to be a repository for words. A second resection was performed based on these findings. The patient experienced no post-operative aphasia and remains seizure free.
3D Rendering + Orthogonal View
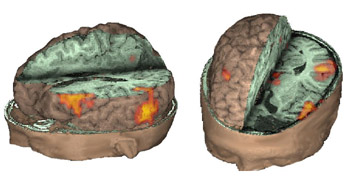
Surface rendering and orthogonal views can be combined in one procedure. This allows us to see activation (or lesions) of the cortex and deep structures of the brain. The bleeding through of activation is obviated. External landmarks of the head and face may also help in surgical navigation.
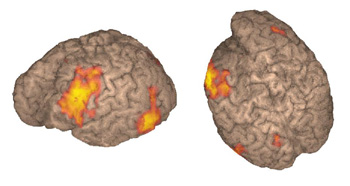
Surface and orthogonal rendering of the brain is viewed in natural anatomical orientation. This means that the structures appear as if they were under direct sight. For that reason the left hemisphere appears on the right side of the left-top-rostral view, and on the left side on the left-top-posterior view. The fMR image presented here depicts activation of the angular gyrus observed in a right-left laterality decision task. The hemi-axial plane shows the activation placed in the deep portion of the left parietal sulcus.
Case 1
11-year-old right handed boy with intractable epilepsy and left hemiparesis. Patient was mapped for language as part of his work up for epilepsy surgery with a "Semantic Fluency Task."
3D-surface rendering and orthogonal views. The images show activation of Broca's area along pars orbitales, triangularis and opercularis in the left hemisphere. Activation is also observed in visual areas likely related to visual strategies. Activation of the basal ganglia is occasionally seen as in this case. Activation can be localized on one image including the cortex, the sylvian fissure, the calcarine fissure, the lateral ventricles and along the midline.
Case 2
Right handed 11 year-old-girl with persistent intractable epilepsy who had a partial left frontal resection . Patient underwent language mapping with fMR.
These images complement case 2 presented in "Surface Rendering." Activation is obtained with a "verb generation" task in Wernicke's area not only along the cortical surface but deep along the gyri.
Case 3
13 year old right handed-boy, with temporal lobe epilepsy. A multicystic oligodendroglioma was found in the left temporal lobe (black arrows). Functional MRI was prescribed to map language areas, prior to surgical resection.
A 3D-fMRI depicts the mass in the left temporal pole. The activation was obtained utilizing a "Repetition Task" paradigm (bubbles in yellow, orange, and red). The relationship between the lesion and the speech areas are beautifully displayed.
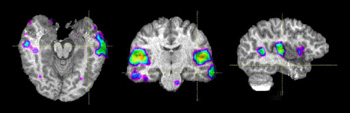
Case 4
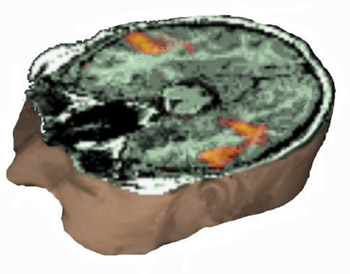
Right handed 19 year-old female volunteer, performing a Stroop-like paradigm. This task involves inhibition, potentially useful in ADHD evaluation.
Activation is located in the cingulate gyrus, right inferior frontal, and supramarginal gyrus (red bubbles). The blue bubble located in the right frontal pole corresponds to inhibited areas. The combination of orthogonal axial and sagittal planes allow simultaneous presentation.
Triple Rendering
The neurosurgeon has a restricted view of the brain through the small window of the craniotomy. Modern neuroimaging can provide anatomy in three dimensions, and a much wider window.
Case 1
27-year-old right handed woman who underwent MRI and MRV to rule out a structural lesion. The patient volunteered to perform a verb generation task.
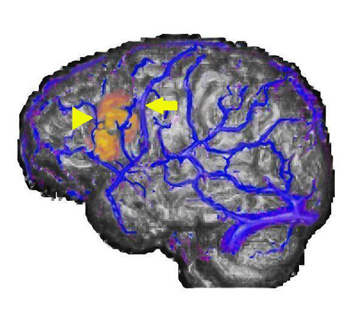
The image shows the fusion of three different procedures. In gray scale is the volumetric rendition of the brain obtained from the MRI sequence. In blue are depicted the surface veins and sinus of the left hemisphere from the MR-venogram. In yellow and red appears activation obtained from the echo-planar sequence used for functional MRI.
Case 2
17 year-old right handed boy with intractable epilepsy of partial motor type. MRI showed signal abnormality in the left middle frontal gyrus consistent with cortical dysplasia.
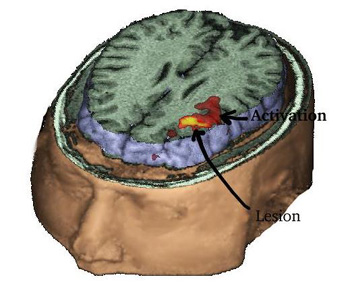
MRI of the head with partial exposure of the brain and skull. An axial view located at the superior third of the inferior frontal gyrus demonstrates in red the activation obtained with a verb generation task. The yellow spot represents the lesion and is derived from a fluid attenuated inversion recovery (FLAIR) sequence, and rendered with the rest of images, revealing the relationship between the lesion and the eloquent areas.
Case 3
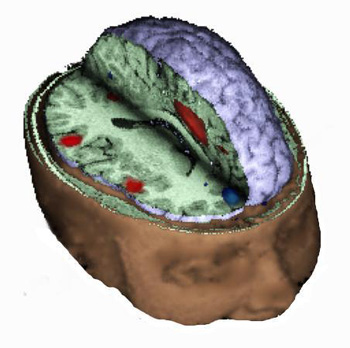
15 year-old right handed girl with sensory-motor partial seizures involving the left hand since the age of 5. MRI showed a focal signal abnormality in the right postcentral gyrus consistent with a developmental tumor without changes over 2 years.
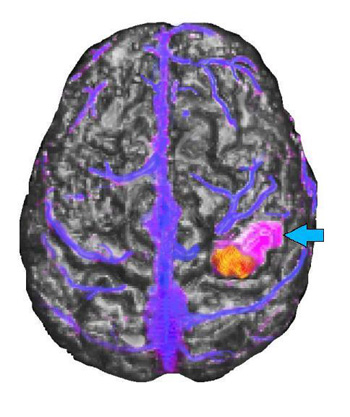
MRI of the brain appears in gray scale, functional MR activation is in yellow and red, the tumor is purple (light blue arrow), and the veins are blue. The tumor appears located in the post-central gyrus lateral and rostral to the functional activation. The relationship between the tumor and the functional activation was confirmed during awake intraoperative mapping. The venous landmarks provided useful information to the operating surgeon. The patient's tumor was removed without residual monoplegia. The patient had only transient loss of stereognosis and proprioception involving the 3rd, 4th, and 5th fingers, post-operatively.